


Editor’s note: In this second of a two-part series, the authors review best management and prevention practices for subclinical hypocalcemia. Click here to read the first-part of the series, Managing hypocalcemia in dairy cows.

Given the high prevalence of subclinical hypocalcemia (SCH) and the high losses associated with this disease, the focus must be on prevention. There are two main approaches to prevention of SCH – dietary manipulation pre-calving and strategic oral calcium supplementation post-calving.
Neither approach is sufficient by itself to prevent all of the negative impacts of SCH; however, using both approaches together will minimize the impacts of SCH as much as possible.
The traditional method of preventing SCH has been to restrict calcium intake during the dry period. However, dietary calcium must be reduced to extremely low levels (less than 20 grams of available calcium per day) for this approach to work. This is not a practical approach for confinement dairy operations but may be more practical under grazing situations.
Supplementing magnesium in prefresh diets also reduces the risk for SCH. Magnesium is necessary for parathyroid hormone secretion and enhances tissue responsiveness to parathyroid hormone.
Dietary acidity or alkalinity prior to calving is the most important dietary means of controlling SCH. Diets relatively high in chlorine or sulfur compared to sodium and potassium invoke an acidic response in the cow and reduce the risk for SCH.
Inversely, diets relatively high in sodium or potassium cause an alkaline response in the cow and increase the risk for SCH. The mechanism for this effect is that an alkaline response by the cow blunts the cow’s responsiveness to PTH, leaving it less able to mobilize bone calcium or absorb dietary calcium.
The measure of the amount of chlorine and sulfur in a diet relative to sodium and potassium is called dietary cation-anion difference (DCAD). Prefresh diets are made lower in DCAD by supplementing anionic salts or by including feed ingredients containing mineral acids such as hydrochloric acid.
Even aggressive use of low-DCAD diets reduces but cannot fully control SCH in a dairy herd. Thus, oral calcium supplementation post-calving is an essential component for optimal control of SCH.
The best oral calcium sources are acidogenic salts such as calcium chloride and calcium sulfate. These salts provide additional calcium for absorption from the gut plus extend the time period the cow is in a relatively acidic state.
Because calcium chloride and calcium sulfate invoke an acidogenic response in the cow, this enhances the cow’s responsiveness to PTH and improves its ability to mobilize calcium from the cow’s own bone.
It is important to understand oral calcium supplementation improves blood calcium concentrations but does not fully restore all cows to normal levels. Nonetheless, providing a burst of blood calcium from oral supplementation after calving does help mitigate the negative impacts of SCH on health and productivity.
It also does not appear to interfere with the cow’s own natural efforts to increase mobilization of bone calcium.
Cows supplemented with oral calcium after calving use most of the extra calcium provided to make more milk. They do this at the expense of maintaining normal blood calcium. This highlights the cow’s amazing biological drive to produce milk, even at the risk of its own well-being.
Best economic response to oral calcium supplementation is in high-producing and lame cows
We undertook a very in-depth evaluation of the economic impact of oral calcium supplementation strategies in dairy herds. Each strategy involved giving one calicum bolus (Bovikalc) at calving and a second bolus the day after calving. Only second-lactation-and-greater cows were supplemented. A summary of the expected economic returns from different supplementation strategies is shown in Figure 1.
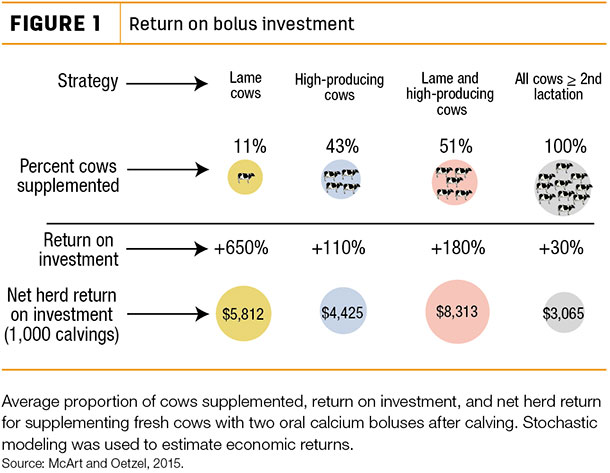
The strategy that had the greatest net return to the herd was supplementing lame and high-producing cows. By following this strategy, a dairy producer would supplement 51 percent of fresh cows, and the average return on investment would be 180 percent (i.e., an investment of $1 would return the $1 invested plus an additional $1.80).
High-producing cows were defined as cows above 105 percent of herd average milk production.
Supplementing only the lame cows had a very high average return on investment (650 percent) but involved supplementing only 11 percent of the eligible cows. Because fewer cows were supplemented, the average net herd return from this strategy was less using this approach compared to supplementing both the lame and high-producing cows.
Supplementing all second-lactation-and-greater cows with two boluses gave a 30 percent return on investment (i.e., each $1 invested returned the $1 plus an additional 30 cents). Since this approach involves supplementing all cows, the average net herd return was substantial but was lower than if only the high-producing and lame cows were supplemented.
An advantage to supplementing all cows is: It is a much simpler strategy to implement. It does not require locomotion scoring or creating a list of cows by milk production.
There are two key limitations to controlling SCH in dairy herds. One is that overuse of anionic salts or acidogenic oral calcium supplements will cause too much of an acidic response in the cow.
Excessive acidosis makes the cow feel sick and lowers appetite. The other limitation is that alternate, non-acidogenic sources of calcium such as calcium propionate could raise blood glucose too much. If blood glucose is elevated too much (hyperglycemia), then abomasal motility and appetite could be impaired.
It is biologically impossible to entirely eliminate SCH from a dairy herd using current technologies. The cow’s remarkable biological drive to produce milk and the limitations of acidosis and hyperglycemia cannot be fully overcome. However, we can minimize losses from SCH by correctly using the tools we have available.
Take-home points
- Take subclinical hypocalcemia seriously.
- Work with your veterinarian to screen a sample of cows for blood calcium concentrations on the day after calving.
- Utilize both dietary manipulation and oral calcium supplementation as a means of optimally managing subclinical hypocalcemia.
- Target high-producing and lame cows for oral calcium supplementation after calving.
References omitted but are available upon request. Click here to email an editor.
—Submitted by Boehringer Ingelheim Vetmedica






